


Surgical treatment of stone disease in children
Childhood stone disease is an important health problem, and it is an important disease that should be diagnosed and treated carefully, especially in regions such as Turkey where it is common. There are many treatment options in the surgical treatment of these stones. These are breaking of stones with shock waves created outside the body (SWL), stone treatments performed by entering the urinary canal (ureterorenoscopy, retrograde intrarenal surgery), percutaneous stone surgery by reaching the kidney from the skin, and open stone surgery.
Stone breaking with external shock waves (SWL)
It is a treatment method based on the principle of shock waves sent from outside the body hitting the stone and causing less damage to the surrounding tissues, unlike open surgery. During this process, the stones break into small particles and become easily excreted in the urine .
In children, this procedure is performed under general anesthesia. Today, approximately 85% of stones requiring active treatment can be treated with SWL. SWL is recommended for upper and middle ureteral stones and kidney stones up to 2 cm.
This treatment option has some potential risks. These; Pain during the passage of broken stone fragments, if the urinary flow is obstructed during the progression of the stone from the ureters, the need for closed method (ureterorenoscopy) cleaning of these stone fragments, it may cause urinary tract infection, it may cause bleeding into or out of the kidney capsule (1-13%), bruising, redness and pain, slight bleeding in the urine that can last up to 1 day, deterioration in heart rhythm due to shock waves, and mild tissue damage to the kidney, adjacent organs and tissues can be counted.
It is not a suitable treatment option for some patients. These; Those who have bleeding disorders or use blood thinners, those with urinary tract infections, those with aortic and renal artery (renal artery) aneurysm (ballooning) and renal artery calcification (calcium precipitation in the vessel wall), those with significant skeletal disorder or overweight, those with a pacemaker SWL should not be applied in patients with heart rhythm disorders and in case of obstruction below the stone to be broken.
Endoscopic (ureterorenoscopic) stone removal
Ureterorenoscopy (URS) means the examination of the upper urinary system (ureter and renal collecting system) with endoscopic devices. The device used for this procedure is called a ureterorenoscope: With this optical instrument, the stone is reached from the urethra to the bladder and from there to the ureter and kidney, and the stone is broken by various methods (usually laser source is used) and the patient is freed from the stone. The device used here may be rigid (figure 2).
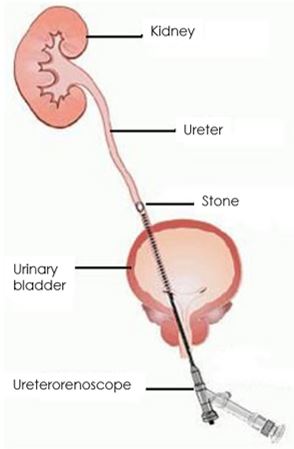
Figure 2: Reaching the stone by rigid ureterorenoscope.
If the stone is in the upper ureter or kidney, flexible ureterorenoscopes are used (figure 3). This method is also called retrograde intrarenal surgery (RIRS)(figure 4).
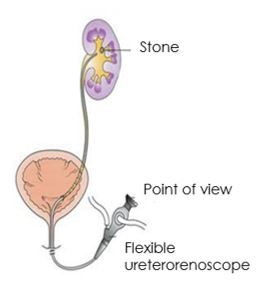
Figure 3: Reaching the stone in the kidney with a flexible ureterorenoscop
At the end of the operation, a ureteral catheter, or a soft plastic thin tube (JJ catheter, stent) with one end in the kidney and the other end in the bladder is inserted into the ureter. This stent will contribute to the presence of the stone in the ureter and the healing process of the trauma associated with the removal of the stone. A Foley catheter is attached to the bladder. The catheter can be withdrawn after the urine color clears within 24-48 hours after the surgery. Removal of the stent takes 2-4 weeks.
Sometimes difficult situations may be encountered during the operation. The stone may not be reached, the ureter may not be entered, and a tear may occur in the ureter. In such cases, after a stent is placed in the ureter and the system is relaxed, ureterorenoscopy is performed again in another session. In cases where a stent cannot be inserted, an external tube may be inserted into the kidney by a procedure called percutaneous nephrostomy to relieve the kidney. In cases where the trauma to the ureter is very large, it may be necessary to complete the procedure with open surgery.
Complications that may develop due to ureterorenoscopy in the long term; stenosis at the ureterovesical junction (where the upper urinary tract connects to the bladder) and vesicoureteral reflux (backflow of urine from the bladder to the kidney). Stenosis has been reported in 1-2% of large series. It is often caused by improper healing of traumatic tears caused by the passage of metal instruments through the ureterovesical junction. Endoscopic expansion may be an option in the treatment, but some patients may require correction with open surgery. Vesicoureteral reflux, which may develop for similar reasons, rarely requires surgical intervention. It is often a low-grade condition that has the potential to heal without the need for treatment.
Percutaneous nephrolithotomy (PCNL)
SWL is often insufficient in children with high stone burden, in those with lower calyx (intrarenal collecting pool) stones that cannot be removed with SWL, and in structural and anatomical disorders of the kidney (horseshoe kidney, double collecting system kidney, etc.). In this case, percutaneous nephrolithotomy is recommended primarily.
With this technique, the kidney is reached with a 1 cm incision from the skin and the stones are broken and taken out. PCNL operation is performed under general anesthesia and takes an average of 1.5-3 hours. Following the administration of anesthesia, the patient is first positioned for the cystoscopy procedure. After the opening of the canal of the stony kidney, which is planned for the operation, is determined, a thin tube with two open ends is placed in this canal. The patient is then placed in the prone position (figure 5).
After positioning the patient, contrast material is given through the catheter inserted during the cystoscopy procedure and the kidney is visualized. According to the location of the stone to be cleaned, an instrument called a nephroscope is inserted into the kidney from the patient's back region (figure 6).
After the stones in the kidney are detected, they are broken in the kidney with various energy sources. These small pieces of broken stone are taken out of the body with the help of a holding tool (figure 7).
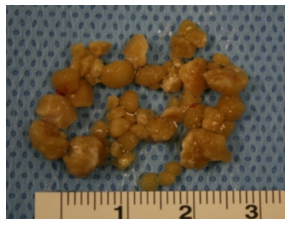
Figure 7: Stones broken and removed by percutaneous nephrolithotomy.
Considering that the kidney is completely free of stones, a tube (percutaneous nephrostomy tube) is placed in the operated kidney. Patients exit the operation with a catheter and a percutaneous nephrostomy tube. The patient's catheter is usually taken on the 1st day after the operation. The patient's percutaneous nephrostomy tube is usually taken at the bedside 2 days after the operation. After the percutaneous nephrostomy tube is removed, the patient is usually discharged on the same day.
This surgery has shorter hospital stay, recovery times, need for painkillers and return to daily life, and its cosmetic appearance is better than open surgery. Patients spend the postoperative period much more comfortably than open surgery. When this method is applied alone and in a single surgical session, stone-free success rates vary between 87 and 98%. In addition, it is known that these success rates increase when the second session or ureterorenoscopy or SWL is added to the treatment.
Open surgery
In the presence of stones that cannot be treated with other treatment methods, in the presence of stonesin congenital anomalies such as ureteropelvic junction obstruction, in the presence of complex calyx (intrarenal collecting pool) anatomy, in cases with severe skeletal disorders, open stone surgery may be required. Removal of kidney stone by open surgery is a surgery that can be performed under general anesthesia. The operation is performed with an incision parallel to the ribs 1-2 cm below the ribs by giving a special lateral position (lumbar position). The stones are removed by opening the kidney by cutting the fleshy part of the kidney that produces urine (nephrolithotomy) or the pool where the urine is collected (renal pelvis) (pyelolithotomy) or a combination of the two. A catheter may be placed in the urinary canal during the healing process of the kidney. A catheter is placed in the bladder at the beginning of the operation and a drain is placed in the operation area at the end of the operation. Due to the widespread use of both SWL and other treatment methods (such as percutaneous stone surgery, flexible ureterorenoscopy), the need for open stone surgery has decreased to 1-2% today.